Why Do Smart Clinicians Make "Obvious" Mistakes?
They usually don't. We just think they do.
First, something uncomfortable:
When we review adverse events in clinical medicine, we are not as objective as we think we are. We believe we are analysing what happened. What we are actually doing is reconstructing it — backwards, through the filter of an outcome we already know — and calling that analysis.
That distinction matters more than most of our safety culture currently acknowledges.
Two Views of the Same Decision
Picture this. A frail, elderly patient arrives with a dislocated hip. The team needs to reduce it. General anaesthesia is the guideline-aligned choice — but this patient is hemodynamically fragile, cognitively impaired, alone. The anaesthesiologist weigh it up. She choose procedural sedation. She balance one set of risks against another, using their experience, reading the patient in front of them, working with what the system is offering at that moment.
If it goes well: nothing. The case closes. Nobody writes it up.
If complications arise: suddenly that same decision — identical in its original logic — becomes a deviation. A lapse in judgement. Something that should have been obvious to avoid.
The decision did not change. The knowledge around it did.
This is the central problem. And it is one that most of our incident review processes, our M&M meetings, our debriefs — are structurally designed to ignore.
The Problem Has a Name
Hindsight bias is not a personality flaw or a failure of professionalism. It is a feature of human cognition, documented robustly in psychological research: knowing an outcome systematically changes how we perceive the events that preceded it (Fischhoff, 2003; Kahneman, 2013). Ambiguous signals start to look diagnostic. Alternative paths appear clearly visible. The correct action seems obvious.
But here is what that research also tells us: those signals were not obvious at the time. They were ambiguous, weak, buried in noise. The meaning we now assign to them was constructed after the fact, not available before it (Klein, 2011).
We are not seeing more clearly in retrospect. We are seeing something fundamentally different.
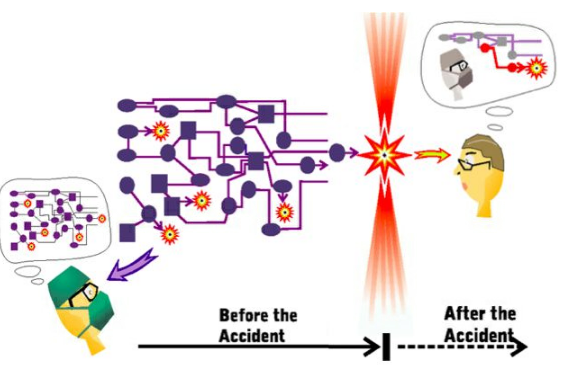
Dekker (2014) calls this the asymmetry between the forward view and the backward view. In real time, clinicians act prospectively — within a system that constrains and shapes their options, under time pressure, with incomplete information, making the most plausible call available. In review, investigators work retrospectively — with known outcomes, simplified causality, and a cognitive architecture that makes prevention feel like it should have been straightforward.
These are not two versions of the same event. They are two different epistemic positions. Treating them as equivalent is where our learning breaks down.
What This Means for Prehospital and Acute Care
In environments like HEMS and prehospital emergency medicine, this is not abstract. It is operational.
Every shift involves decisions made under conditions that are the opposite of ideal: incomplete patient history, environmental constraints, limited team resources, time pressure that is not metaphorical but physiological. Pattern recognition — what Klein (2011) calls recognition-primed decision making — is not a shortcut. It is the appropriate cognitive tool for that environment. Experts do not optimise between multiple explicit options. They recognise a plausible course of action and run a mental simulation: will this work? If yes, they act.
That process looks, in hindsight, like it bypassed steps that should have been taken. It didn't. Those steps weren't available in the same form. The situation was different from the inside.
Rasmussen (1997) gives us the framework to understand why: practitioners don't operate in open space. They navigate within boundaries — efficiency, safety, workload, resources — that are constantly shifting. Behaviour that drifts toward a boundary isn't reckless. It is the system adapting to its own constraints. And that same adaptation is what keeps the system functioning the vast majority of the time.
When we call that adaptation an error after the fact, we are not learning from the case. We are prosecuting it.
The Workaround Problem
There is a related issue that clinical educators and safety officers need to sit with.
Workarounds — the modifications practitioners make to procedures, workflows, or protocols when the designed system does not match operational reality — are almost universally treated with suspicion. The assumption is that they represent deviation, carelessness, or non-compliance.
The evidence from resilience engineering says something quite different.
Woods et al. (2021) argues that systems do not function because people follow procedures. They function because practitioners actively adjust performance to meet conditions the procedures didn't anticipate. Those adjustments — the workarounds — are not the exception. They are the normal operating mode of any complex adaptive system.
Here is the uncomfortable implication: the adaptive process that contributes to success on Monday is the same process that gets labelled as the cause of failure on Friday. The difference is the outcome, not the behaviour.
A workaround that works is invisible. A workaround that coincides with harm becomes, in retrospect, a deviation. This is not analysis. It is outcome-driven narrative construction — and it actively distorts our ability to improve.
What We Should Be Asking Instead
Traditional clinical debriefs and incident reviews are organised around a version of the same question: What went wrong?
It feels rigorous. It feels like accountability. But it imports hindsight bias directly into the conversation — because the answer is always constructed from a position of outcome knowledge.
The more useful question — harder to ask, more uncomfortable to sit with — is: Why did it make sense at the time?
That question forces you into the forward view. It asks you to reconstruct the situation as the practitioners experienced it: what they could see, what pressures they were navigating, what the system was offering them. It treats behaviour as a product of conditions, not just of character.
This is not about lowering the bar for accountability. It is about directing accountability at the right level. If a decision made sense given the conditions, the question becomes: what conditions need to change? That is a systems question. That is where sustainable improvement lives.
The Implication for Education
As educators, we have a specific responsibility here — because how we teach people to analyse performance shapes how they will analyse it for the rest of their careers.
If we consistently debrief from outcome backwards, we train clinicians to believe that good decisions are the ones that worked, and poor decisions are the ones that didn't. We inadvertently build a culture where the lesson of an adverse event is: next time, be smarter. Which is no lesson at all.
The Honest Conclusion
The question is not why smart clinicians make obvious mistakes.
The question is why we keep insisting the mistakes were obvious — when the people who lived through the situation, with the information they had, in the system they were operating within, made decisions that were entirely coherent at the time.
That insistence costs us something real. It produces cultures of individual blame rather than systemic insight. It makes people less likely to report near-misses. It focuses improvement energy on human performance rather than on the conditions that shape it.
HFSS does not excuse poor practice. It asks us to understand what produces it — which turns out to be a much more difficult and more important question.
The past was never as clear as it looks from here. The sooner we build that into how we investigate and how we teach, the better our patients will be.
Conceptual framework from: Dekker (2002, 2014), Rasmussen (1997), Klein (2011), Woods et al. (2021), Fischhoff (2003), Kahneman (2013).